| Department of Pathology, State University of NewYork at Stony Brook |

 Go to: TOC |
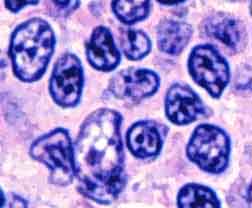
RIGHT off the bat it should be said that lymphomas of follicular center cell origin may have follicular or diffuse growth patterns, or both. In cases of purely diffuse growth, the follicular origin may be inferred from a combination of soft signs: immunophenotype (CD10+), cytogenetic (t[14;18]), and morphologic (the presence of small cleaved B-cells).
The follicular pattern must be distinguished from other benign and malignant nodular processes, including:
One of the more difficult morphologic distinctions in hematopathology can be between reactive follicular hyperplasias and follicular lymphomas. The important points include: |
|
|||||||||||||||
|
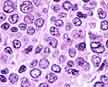
Subtypes of Follicular Lymphoma Follicular lymphomas are divided into 3 types according to the ratio of small-cleaved and large cells:
As with many cancers, follicular lymphomas tend to become more aggressive with time. The percentage of small-cleaved cells may decrease, and the nodularity may grow fainter or vanish. As the proportion of large cells increases, so does the mitotic rate, the tendency to grow diffusely, and the aggressiveness of the lymphoma. In addition, the BCL-2 gene rearrangement is found less frequently. It seems a little mysterious that follicular lymphomas may develop a diffuse growth pattern, but that is part of their malignant potential. As malignant follicular center cells begin to dedifferentiate, they lose their ability to ape the appearance and behavior of their normal counterparts. Treatment options depend on the stage and grade of the disease. The infrequent patients with early-stage disease may be treated with local radiation, with or without chemotherapy. Patients with more advanced but low-grade disease may remain untreated as long as no symptoms or lymphoma-related organ compromise are present. When treatment becomes necessary, the options include: 1) single-agent alkylator therapy; 2) low-intensity combined chemotherapy without an anthracycline; 3) whole-body irradiation. Large-cell follicular lymphoma is classified as an intermediate-grade lymphoma, and the patients may benefit from the inclusion of an anthracycline in their chemotherapy. Extranodal Involvement

Follicular lymphomas are reactive for pan-B-cell markers CD19, CD20, and CD22 in addition to expressing monoclonal light chains. Most cases also react for CD10, which is also seen in lymphoblastic lymphoma but not other low grade lymphomas. No staining for CD5 is seen. Most cases of follicular lymphoma, especially those rich in small-cleaved cells, have a t(14;18) translocation. This results in a rearranged and constitutively over-expressed gene called BCL-2. The BCL-2 gene product is an inner mitochondrial membrane protein that blocks apoptosis (in plain English, programmed cell death). Although this protein is produced by an unrearranged BCL-2 gene in much benign lymphoid tissue and many lymphomas besides follicular ones, it is not detected in benign, reactive germinal center cells. Thus its presence, as detected by immunostaining, can differentiate malignant from benign follicles.

|