
Go to:

TOC
Prev
Next
|
Diffuse Intermediate Grade Lymphomas and Immunoblastic Lymphomas
Mixed lymphoma | Large
cell lymphoma | Immunoblastic lymphoma
THIS category includes:
- Diffuse mixed small and large cell lymphoma (either of follicular center
cell or uncertain origin)
- Diffuse large cell lymphoma
- Immunoblastic lymphoma
Because follicular large cell lymphoma was discussed previously as a
follicular lymphoma, this section omits it although it too belongs to
the Working Formulation intermediate grade. Also, the original Working
Formulation classified immunoblastic lymphoma as high grade. Subsequent
experience, however, has shown that all three of lymphomas listed above
show little difference in prognosis; moreover, even veteran hematopathologists
may disagree about classifying particular cases as immunoblastic or large
cell. For these reasons, diffuse large cell and immunoblastic lymphomas
are discussed together here as elsewhere
Aggressive histology
| .
With this section
we step gingerly into the territory of lymphomas that are
aggressive in histology and clinical behavior. Aggressive histology means
that many of the lymphoma cells are highly atypical: large and irregular,
with vesicular nuclei and prominent nucleoli. Aggressive behavior means
that, untreated, these lymphomas kill patients in 1-2 years. With contemporary
chemotherapy, however, 50% of the patients have long-term, disease-free
survival; and the lucky ones can be cured.
Diffuse
Mixed Small and Large Cell Lymphoma
Diffuse mixed lymphomas
(images) comprise 7% of all non-Hodgkin's lymphoma, with
a median age of 58 and a range of about 20-70 years of age. Extranodal
involvement is seen in 60% of cases, including the bone marrow in 14%. mixed lymphomas
(images) comprise 7% of all non-Hodgkin's lymphoma, with
a median age of 58 and a range of about 20-70 years of age. Extranodal
involvement is seen in 60% of cases, including the bone marrow in 14%.
Diffuse mixed lymphomas
may originate from follicular center cells (by the way, low grade follicular
lymphoma has a slightly different name that includes
the word "cleaved": follicular small-cleaved and large
cell). Evidence for a follicular nature includes:
- The presence of small-cleaved cells.
- A small component with a follicular growth pattern.
- Cytogenetically the BCL-2 gene rearrangement: t(14;18).
- Reactivity for CD10 (pretty soft evidence).
Cases of follicular origin tend to occur in younger patients and behave
more like indolent diseases: survival is longer, and the response to treatment
does not significantly affect it.
Diffuse
Large Cell Lymphoma
This is

Diffuse large cell lymphoma in spleen
|
one of the most common types of lymphoma (images), comprising about 20%
of non-Hodgkin's lymphomas. The median age is 57, with a range of 10-88
years. Although most frequently seen in adults, large cell lymphomas are not uncommon in
children.
As aggressive malignancies with a tendency to metastasize, the
majority eventually demonstrate some extranodal component, including the gastrointestinal tract, testes, thyroid, skin, breast, central nervous system or bone. Although generally extra-nodal involvement is more common than in follicular lymphomas, the marrow is involved only about 10% of the time. About 20% of the cases have good evidence for a
follicular center cell origin in the form of a t(14;18), BCL-2
rearrangement.
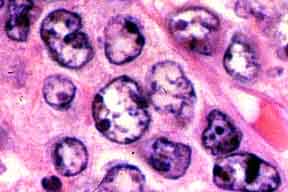
The large cells may be cleaved
or round to oval. The most characteristic cell, called a "centroblast",
has a large, open nucleus with several moderately prominent nucleoli
that apply themselves to the nuclear membrane. About one-third of B-cell diffuse
large cell lymphomas fail to produce surface
immunoglobulin. Fortunately for the diagnostician, these are overt malignancies,
so proving clonality is an academic issue. In the Working Formulation,
this category included some T-cell as well as B-cell lymphomas.
Immunoblastic
Lymphoma
This category includes many cases with very atypical cells. The prototypical
immunoblast (image) is a large cell with reddish-blue ("amphophilic")
 cytoplasm and a large, oval, vesicular nucleus with a single, prominent,
cherry-colored, central nucleolus. The patients' median age is 52 with
a range from 10-81 years of age. One-half have extranodal disease including
marrow involvement in 12%. They account for only 8% of all non-Hodgkin's
lymphomas but a much higher proportion of AIDS-related lymphomas. Another
clinical association is auto-immune disease. cytoplasm and a large, oval, vesicular nucleus with a single, prominent,
cherry-colored, central nucleolus. The patients' median age is 52 with
a range from 10-81 years of age. One-half have extranodal disease including
marrow involvement in 12%. They account for only 8% of all non-Hodgkin's
lymphomas but a much higher proportion of AIDS-related lymphomas. Another
clinical association is auto-immune disease.
Like diffuse large cell lymphomas,
immunoblastic lymphomas are surface immunoglobulin negative one-third of
the time. Their cytoplasm may, however, contain readily detectable amounts
of immunoglobulin. For those of you who are "splitters," the
following subtypes have been defined:
- Plasmacytoid
- Clear cell
- Polymorphous
- Cases with markedly increased numbers of epithelioid histiocytes (some
of which may be seen in other subtypes)
In the Working Formulation, some T-cell lymphomas were included in this
category.

Table of Contents |
Next section |
Previous section
|
