|
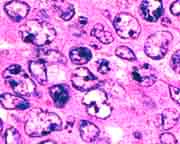
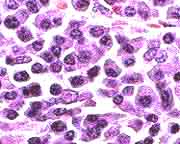
Like carcinomas and sarcomas,
NHLs more or less resemble
the normal tissue from which they derive. What makes life for the diagnostician
more difficult is that normal lymphocytes go through many stages as they
develop from small, resting, inexperienced cells to larger,
atypical-appearing, proliferating cells. The stimulus for this change, of course, is exposure to antigen. Malignancies may arise from lymphoid cells arrested at any of these stages. Morphologically, immunophenotypically, and genetically, the NHLs
fall into categories with important therapeutic
and prognostic associations.
Both cytologically and
architecturally, lymphoid proliferations may lack some of the morphological
complexity seen in more highly structured organs. In some cases, ancillary
laboratory studies are necessary to determine if a lymphoid proliferation
is benign or malignant or to identify its lymphoma subtype. These studies
include:
-
Immunophenotyping
to determine what kind of surface molecules are present on the cells.
-
Cytogenetics to
identify any abnormal chromosomes.
-
Molecular diagnostics
including Southern blotting and the polymerase chain reaction to uncover
clonal rearrangements of immune system genes or other genetic, subchromosomal
evidence of malignancy.
Many attempts
have been made to classify NHLs. Currently the most widely used is
the Working Formulation.
Based on only two criteria--1) the cytologic appearance of individual
cells and 2) the follicular or diffuse nature of the proliferation--
NHLs are named and then categorized as low grade, intermediate
grade, or high grade. These categories have clinical significance that
was demonstrated in an initial study of over a thousand cases. Our discussion
will use Working Formulation terminology, along with additional distinctions
that postdate it.
For the patient and clinician the most important distinction is between low grade NHLs on the one hand and intermediate and high grade ones on the other. These 2 groups of NHLs have morphological, biological, and clinical differences that are discussed later.
Epidemiology:
In the United
States the incidence of NHL in the last few years has been 17.9/100,00 in males and 11.5/100,000 in females. In 1998 an estimated 55,400 new cases will arise, and 24,900 deaths will occur. At this rate, it is the fifth or sixth most common cause of both new cases of cancer and cancer deaths. In comparison, 1998 will see 184,500 new cases of prostate cancer, 180,300 new cases of breast cancer, and 7,100 new cases of Hodgkin's lymphoma. The rate of NHL is twice as high in whites than in blacks.
Since the early 1970's the incidence of NHL has been increasing
at the rate of 3-4% per year, which is impressive even after adjustment for the aging U.S. population and AIDS-related cases. The current aged-adjusted death rate for NHL is about 37% higher than it was 20 years ago, despite improved therapies that allow a 52% five-year survival rate compared to an earlier 41%. Only lung cancer in women and melanomas are increasing more rapidly. Unlike Hodgkin's lymphoma, which has a bimodal age distribution, the incidence rate of NHL steadily and steeply increases after age 30 years, although childhood NHLs are not rare.
The 1980s saw a startling incidence of NHL among patients with AIDS, who have a particularly high rate of high grade, extra-nodal, or central nervous system NHLs. In this setting these types of lymphomas occur
60 times more frequently than in the general population. In one study the rate of NHL, measured from the initiation of zidovudine therapy, was 12% at 2 years and 29% at 3 years.
NHLs are also
very prevalent among patients with primary immunodeficiencies or with therapeutic
immunosuppression such as transplantation regimes. In post-transplant patients,
evidence of clonal Epstein-Barr virus infection can be found in most NHLs.
Besides immunodefects,
risk factors for NHLs are hard to identify. The second strongest risk
factor is a family history of the disease, which entails a 3-4 times greater
risk to relatives. A weaker and not completely persuasive factor is occupational
exposure, especially to pesticides and herbicides. Finally a weak, inconsistent
association has been unearthed between NHLs and hair dye use.

Table of Contents |
Next section |
Previous section
|