Go to:

TOC
Prev
Next
|
Hodgkin Disease Subtypes

A patient of Dorothy Reed.
|
FOUR subtypes are identified, divided into two subgroups.
1) Classic Hodgkin Disease
So-called "classic" HD includes:
- mixed cellularity
- nodular sclerosis
- lymphocyte depletion
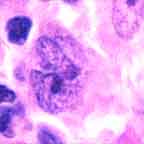
In this group typical
RS cell
|
Reed-Sternberg cells can be found. They are most numberous in mixed celluarity, may be numerous or sparse in nodular sclerosis, and are often bizarre and sarcomatoid in lymphocyte depletion. The Reed-Sternberg cells and variants usually lack surface molecules characteristic of B or T-cells but instead are immunoreactive for CD15 (aka LeuM-1) and CD30 (aka Ki-1) antibodies.
The background lymphocytes are mostly T-cells. Untreated these entities progress to subtypes with increasing numbers of Reed-Sternberg cells. When Hodgkin disease was untreatable, widespread lymphocyte depletion Hodgkin disease with many bizarre Reed-Sternberg cells was often found at autopsy.
Even within this subgroup,
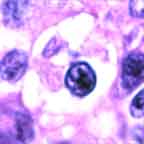
Lacunar cell
|
nodular sclerosis is a bit of a specialty.
It is the only HD subtype more common in women than men, and it very often presents with a mediastinal mass. Named for the dense fibrous bands that subdivide involved lymph nodes, it has a prognosis slightly better than mixed cellularity HD. In formalin-fixed tissue a morphologically variant Reed-Sternberg cell called the "lacunar cell" is found.
As the molecular techniques for probing lineage markers in cells become more refined, new discoveries hint that the Reed-Sternberg cells in most cases of the subtypes of classic Hodgkin disease are derived from B-cells, albeit gravely damaged ones (Schwartz RS. Hodgkin's Disease--Time for a Change. N Engl J Med 1997; 337:495-6).
2) Non-Classic Hodgkin Disease
The other subgroup
has one member: nodular lymphocyte predominance. Because the tumor cells of this subtype have a B-cell immunophenotype (and are negative for CD15 and CD30) and and for other reasons, it has long been suspected of being a kind of B-cell lymphoma. Typical Reed-Sternberg cells are rare to non-existent; instead polylobated variants called L & H cells (colloquially "popcorn cells") are seen. The background lymphocytes are B-cells.
Sometimes the disease is preceded by follicular hyperplasia . Progressive transformation of germinal centers, which usually is not associated with Hodgkin disease, occasionally may precede, accompany, or post-date it . Addtional distinctive clinical features setting apart nodular lymphocyte predominance Hodgkin disease include:
- an indolent though relapsing course with an excellent prognosis;
- occasional cases relapsing as high-grade B-cell non-Hodgkin lymphoma;
- a peak incidence in males in their 30's and 40's, without the bimodal age pattern of classic Hodgkin disease;
- a greater tendency to be restricted to cervical lymph nodes.
Immunophenotype
The immunophenotypes of the Reed-Sternberg cells and variants in the two subgroups of Hodgkin disease are mirror images:
|