| Anorectal Malformation |

 
 |
| Anorectal Malformation |
|
|

|
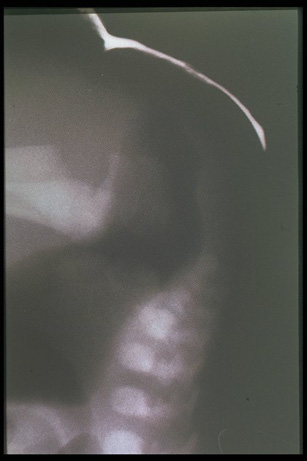
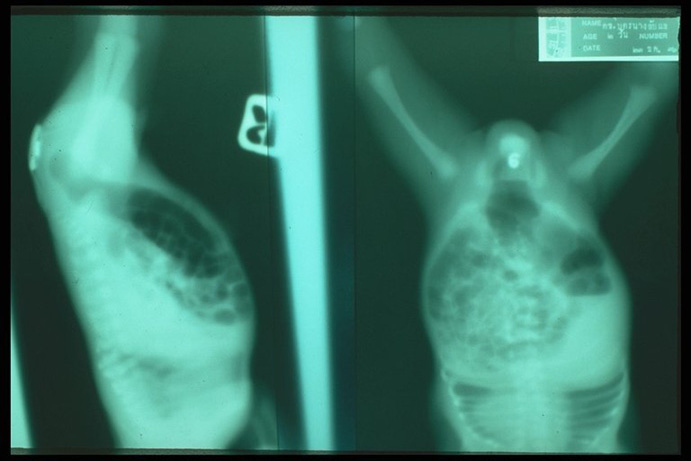
Plain X-ray shows air in the proximal blind pouch indicating Esophageal atresia which is commonly associated with anorectal malformation. A condition that must be excluded before invertogram to avoid reflux of gastric contents through the T-E fistula |
|
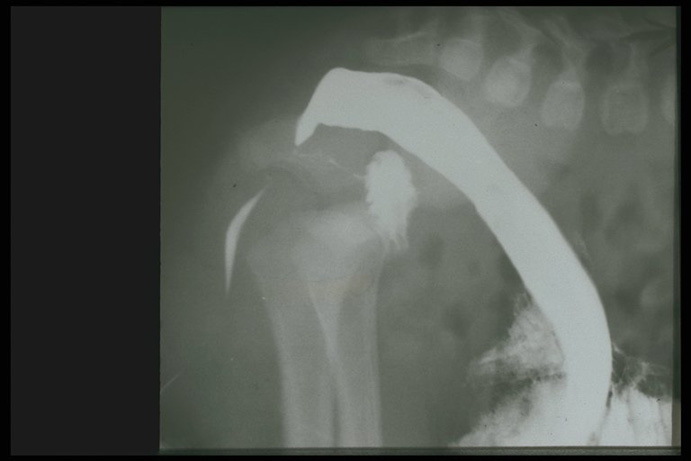
Invertogram demonstrated air in the distal blind rectal pouch, a radiopaque object is placed over the perineum to outline the skin level which is very near to the rectal pouch, low type anomaly can be diagnosed. |
|
|
Invertogram demonstrated air in the distal blind rectal pouch, a radiopaque object is placed over the perineum to outline the skin level which is very near to the rectal pouch, low type anomaly can be diagnosed. |
|
|
Invertogram, lateral view , showed that the distal pouch is not far away from the perineum and also showed the air in the fistula tract in low type malformation |
|
|
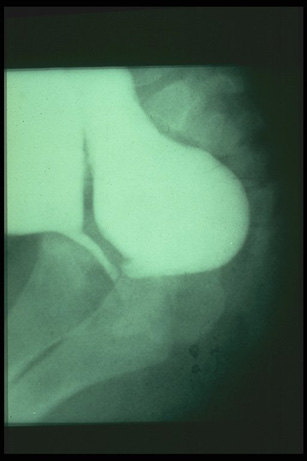
Contrast study demonstrated the fistula tract between the distal rectal pouch and urethra in rectourethral fistula (high type). |
|
|
Distal rectal pouch, urethra, bladder and rectourethral fistula demonstrated by contrast study indicate the high type anomaly |

|
Sacral agenesis or absence of sacrum and coccyx in anorectal malformation. Usually associated with poor neurological control of sphincter |
|
|
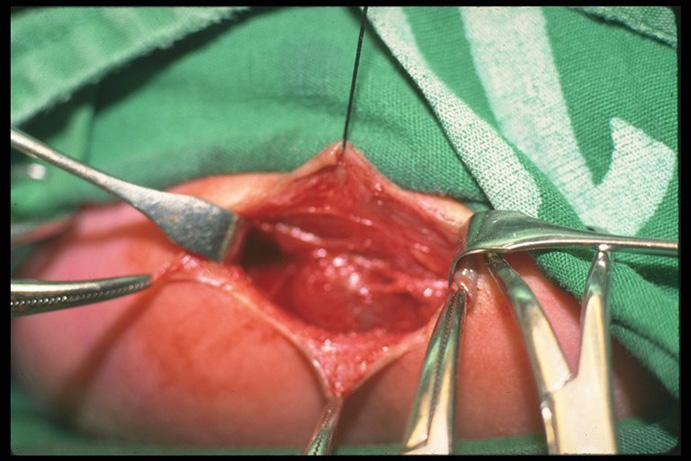
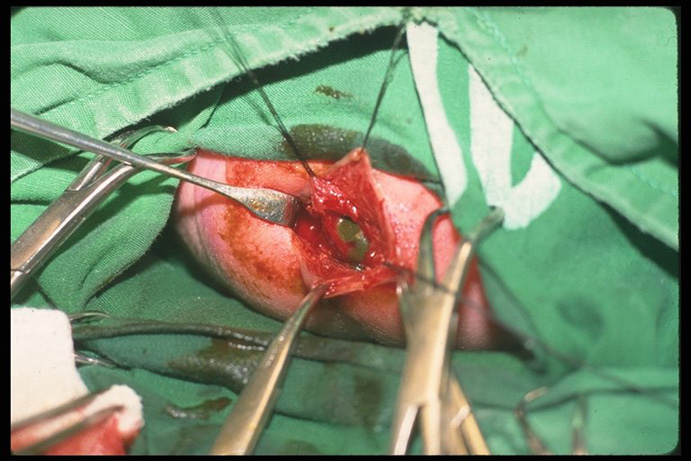
Anoplasty is the operation for low type anomaly, approached through the perineum. The distal rectal pouch is noted |
|
Thick meconium is observed while the distal pouch is open |

|
Colostomy is the initial procedure of choice in high type malformation. Gastrostomy is also performed in a case with associated esophageal atresia |