| Commonly referred to also as "Inflammatory Pseudotumor," the
nature of these myofibroblastic proliferations remains unclear. They often
penetrate deeply into the bladder wall (Fig. 1), but a metastatic potential
has not been reported [4,32,77,85,116,120].
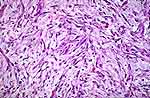
The dominant feature is a spindle-shaped, pink-staining cell suspended in
a myxoid or edematous stroma. The spindle cells are mostly unattached to
adjacent cells, which imparts to the typical microscopic picture a "tissue
culture" appearance (Fig. 2). Where the growth is more compact, fascicles
may be formed and a leiomyosarcoma enters into the differential diagnosis.
Unlike the latter, the pseudotumor frequently contains intermediate filaments
which give a positive reaction to cytokeratin (Fig. 3). Mitoses are frequent
(but not abnormal) and a spindle cell carcinoma is also to be considered.
The latter, with wide sampling, will often reveal an in-situ carcinoma and
epithelial markers (keratin, EMA) will often highlight overlooked foci of
differentiated carcinoma.
The myofibroblastic proliferations in the urethra-bladder neck area
which develops within one to three months after a TUR of the prostate
(postoperative spindle cell nodule) is essentially the same type of lesion
but most of the bladder lesions occur spontaneously. |