| Department of Pathology, State University of New York at Stony Brook |

 Go to: TOC |
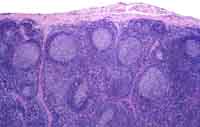
Between the follicles is the parafollicular cortex, called paracortex for short, where the T-lymphocytes live. Also present are the high endothelial venules. These are the vessels from which the vagabond lymphocytes enter the lymph node from the blood. The deep part of the node called the medulla has two elements: 1) the coalescing lymphoid sinuses containing macrophages and scattered lymphocytes and 2) the lymphoid tissue between the sinuses, called the medullary cords (image), which are often the haunt of plasma cells. Let's see what happens to antigens as they enter and trigger a lymph node. The antigen in the lymph stream is carried in an afferent lymphatic channel from its origin in skin lesions, upstream cancers, or other sites. The afferent lymphatic pierces the node's thin fibrous capsule to dump the lymph and its contents into the subcapsular sinus. From there the antigen flows down the trabecular sinuses, which are lymph channels within the node that accompany the fibrous septa called trabeculae. The lymph and the antigens flow toward the hilum, where the lymph node is attached to efferent blood and lymphatic vessels that carry away their respective fluids. As the antigens traverse the sinuses, they are captured and processed by the lining macrophages. Eventually the antigens become available for presentation to the lymphoid cells. The presenting cells are probably the sinusoidal macrophages and, more importantly, dendritic cells that reside either in the paracortex (interdigitating dendritic cells) or the follicles (follicular dendritic cells). Paracortical T-cells, mostly CD4(+) T-helper cells, are key players in the recognition of antigen. They are so tickled by its presence that they communicate their excitement to their B-cell counterparts in the as-yet unstimulated primary follicle.
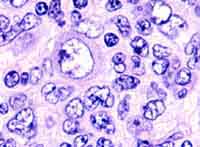
The B-cells that survive the tumultuous, Darwinian struggle within the germinal center eventually differentiate into plasma cells. These minute crafters of antibodies migrate to the medullary cords or leave the lymph node altogether to resettle in the body's distant shores. All this is a dynamic process. Germinal centers appear about a week after the node is challenged by an immunogenic antigen and gradually subside unless further challenged. Other types of reactive lymph node hyperplasia also occur, including hyperplasia of the paracortical region or of the sinus cells, the latter called "sinus histiocytosis" (images). The different kinds of hyperplasias may occur by themselves or in combination.

|