
Go to:

TOC
|
Morphologic Quiz
Obtaining CME Credits |
Registration Form |
CME Quiz Selection | Evaluation Form
Please circle the letter corresponding to the single correct answer for each question. For unfamiliar questions, you might find it helpful to use the Search utility to look up a word or phrase in the tutorial pages.
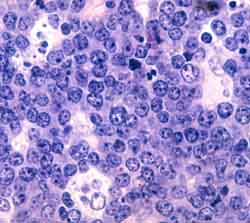
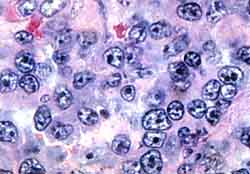
1) In reference to the above image, the best diagnosis is:
- Small non-cleaved cell lymphoma.
- Small lymphocytic lymphoma.
- Lymphocyte predominance Hodgkin's lymphoma.
- Large cell lymphoma.
2) With regard to Hodgkin's lymphoma:
- It is more common than non-Hodgkin's lymphoma.
- Its incidence in the U.S. peaks in 2 different
age groups.
- There is no association with Epstein-Barr virus.
- Its epidemiology is similar in developed and
developing countries.
3) In regard to the age distribution of lymphomas:
- Non-Hodgkin's lymphomas in general are more common
in young adults and children than in older patients.
- Multiple myeloma is primarily seen in older people.
- Indolent lymphomas such as small lymphocytic lymphoma
and follicular small cleaved cell lymphoma are common
in children.
- African Burkitt's lymphoma is primarily a disease of the elderly.
4) A true statement about lymphoma biology is:
- Lymphomas with a follicular growth
pattern tend to be high-grade.
- As opposed to indolent lymphomas, aggressive
lymphomas are incurable.
- The secreted products of lymphoid cells may contribute
to the morbidity of lymphoid malignancies.
- Lymphoma cells have no normal counterparts.
5) The true statement about lymphoid cell behavior is:
- Indolent lymphomas show no response to chemotherapy.
- Indolent lymphomas have no tendency to become
more agressive with time.
- Because plasma cells are terminally differentiated,
there are no plasma cell malignancies.
- Unlike most normal cells, normal lymphoid cells
undergo 2 proliferative, blastic bursts as they mature.
6) A true statement about lymphoma pathogenesisis is:
- Viruses, but not bacteria, have been implicated
in lymphoma pathogenesis
- Any monoclonal plasma cell population in the
marrow is diagnostic for multiple myeloma.
- Exposure to occupational toxins plays an major
role in causing lymphomas.
- Two of the biggest risk factors for lymphoma are
immunodefects and a family history of the disease.
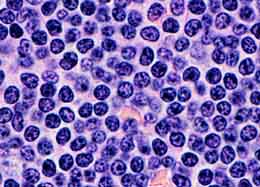
7) In reference to the above image, the feature that might help establish
that it represents part of a malignant follicle is:
- The presence of small-cleaved cells.
- The presence of a larger cell.
- The absence of tingible-body macrophages.
- The absence of plasma cells.
8) A true statement related to lymphoma classification is:
- Immunophenotyping, cytogenetics, and molecular techniques
may all play a role in classifying lymphomas.
- Currently morphologic analysis has been supplanted
by more scientific methods.
- In the Working Formulation, diffuse large-cell lymphoma
is high-grade.
- Nodular lymphocyte predominance is a subtype of
classical Hodgkin's lymphoma.
9) The immunology of non-Hodgkin's lymphoma:
- Kappa:lambda light chain ratios help identify T-cell lymphomas.
- Immunohistochemistry, immunofluorescence, and
flow cytometry are all ways of identifying antigens on a cell.
- Typical B-cells are positive for CD2, CD3, CD5, and CD7 antigens.
- Typical T-cells are positive for CD19, CD20, and CD22 antigens.
10) In regard to laboratory techniques for lymphoma diagnosis:
- A kappa:lambda ratio markedly different
than 2:1 is suggestive of a benign, polyclonal lymphoid proliferation.
- CD (Cluster Designation) numbers are alternative names
for different types of lymphomas.
- An immunophenotype of a lymphoma is description of the antigens
that the lymphoma characteristically does and doesn't express.
- Clonal rearrangements of immunoglobulin or T-cell receptor
genes are usually detected by conventional cytogenetics.
11) The correct association is between:
- a rearrangement involving CyclinD1/BCL-1/PRAD-1
(different names for the same gene) and small lymphocytic
lymphoma.
- an 8:14 translocation of the c-myc gene
and anaplastic large cell lymphoma.
- a 14:18 translocation of the bcl-2 gene
and follicular lymphoma.
- a 2:5 translocation and Burkitt's lymphoma.
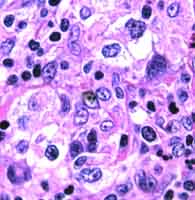
12) In in reference to the above image of a formalin-fixed mass, the large cells with contracted or apparently absent cytoplasm suggest the following subtype of Hodgkin's disease:
- Nodular sclerosis.
- Nodular lymphocyte predominance.
- Mixed cellularity.
- Lymphocyte depletion.
13) A true statement about lymphoma cells is:
- Small-cleaved cells are seen mainly in small lymphocytic
lymphoma
- Lymphoblasts have large, eosinophilic nucleoli.
- The plasma cells in multiple myeloma always appear mature.
- A diagnostic Reed-Sternberg cell has multiple
nuclei with huge, red nucleoli.
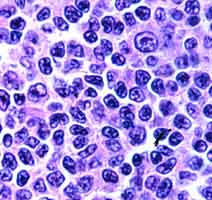
14) In reference to the above image:
- It is sufficient evidence for a diagnosis of lymphoma.
- It is consistent with a diagnosis of small lymphocytic
lymphoma.
- The cells are small-cleaved cells.
- The cells probably represent a high-grade lymphoma.
15) Concerning lymphoma architecture:
- A "starry sky" background is traditionally
associated with Burkitt's or small non-cleaved
cell lymphoma.
- Lymphoepithelial lesions in the GI tract are
associated with T-cell lymphoma.
- All lymphomas with a follicular growth pattern
are low-grade by the Working Formulation.
- Mycosis fungoides cells are confined to the dermis.
16) In Hodgkin's lymphoma as opposed to non-Hodgkin's lymphoma:
- Extranodal involvement is more frequent.
- Indolent cases are not always treated.
- The bulk of the mass consists of reactive, inflammatory cells.
- Immune deficiencies are usually humoral in nature.
17) In higher grade lymphomas (intermediate and high grade) as opposed to
low grade lymphomas:
- Peripheral blood lymphocytosis is more common.
- Extranodal involvement is less common.
- Patients present more often with generalized lymphadenopathy.
- Nuclei are large with open or clear chromatin.
18) In B-cell lymphomas as opposed to T-cell lymphomas:
- Types include mycosis fungoides.
- Immunologically clonality can be demonstrated only by the
abnormal absence of an antigen expressed on all normal B-cells.
- B-cell lymphomas are slightly less common.
- The pan-B-cell antigens CD19 and CD20 are
usually present.
19) In regard to follicles in follicular lymphoma as opposed to a reactive
germinal centers:
- Malignant follicles usually have a higher mitotic rate.
- Malignant follicles have thickened mantle-cell zones.
- Malignant follicles are more densely packed and monomorphic.
- Malignant follicles contain more tingible-body macrophages.
20) In regard to reactive lymph nodes:
- Lymph nodes involved by sarcoidosis feature necrotizing
granulomas.
- Follicular hyperplasia, epithelioid histiocytes,
and moncytoid B-cells characterize nodal toxoplasmosis.
- "Cat-scratch" disease is a misnomer, since in fact
the disease is transmitted by dog-bites.
- The initial change seen in lymph nodes of patients with
AIDS is lymphocyte depletion.
21) With monoclonal gammopathies of undetermined
significance:
- A stable M-component < 3 grams/deciliter
helps to exclude multiple myeloma.
- A marrow plasmacytosis > 25% helps to exclude
multiple myeloma
- In most cases a bone marrow biopsy should follow
the discovery of an M-component.
- Unlike multiple myeloma, the gammopathies tend
to occur in a young population.
22) In Hodgkin's lymphoma, the correct association is between:
- "Popcorn" or L&H cells and nodular sclerosis.
- Lacunar cells and mixed-cellularity.
- More common in women and lymphocyte depletion.
- B-cell immunophenotype and nodular lymphocyte predominance.
23) In a normal, reactive lymph node:
- The follicles are located in the medulla.
- B-cells are found preferentially in the paracortex.
- A secondary follicle consists of a pale germinal center
and a dark mantle zone.
- Antigen enters the node at the hilum.
24) In reference to the above image, the best diagnosis is:
- Hodgkin's lymphoma.
- Lymphoblastic lymphoma.
- Sarcoid.
- Large cell lymphoma.
25) About low-grade, diffuse, B-cell lymphomas:
- "Waldenstrom's macroglobulinemia" is another
name for IgG-secreting plasmacytoid lymphomas.
- Gastric MALT lymphomas are associated with
H. pylori infection.
- Mantle cell lymphoma has a better prognosis than
most diffuse, low-grade lymphomas.
- Diffuse, low-grade lymphomas require agressive
initial treatment.

Table of Contents 
|

